
This system paper gives a “preview” regarding the roles performed by the Information and Communication Technology (ICT) in both developed and developing countries. It will provide an analysis regarding the performance of ICTs and it will also provide a case of evidence where their performance in the developing countries is explained. The theory which is taken into consideration is the design-reality gap analysis which is used to observe the gaps in the design and the current reality of the country. It draws from the experience of utilisation
in both the developing and developed states. In this advanced age, information and communication technologies (ICTs) are thought to be the ‘impetuses to improvement. There are numerous studies which exhibit that information systems can make important contribution to the health sector, especially in the essential health-care.
The beginning stage of the health projects is the change of health-care services utilising ICT. Enhancing data diverts in rustic groups can have a gigantic effect on sicknesses, for example, HIV/AIDS, jungle fever, the runs and water-related ailments, all of which are keeping on having a staggering effect upon the strength of the country populaces in developing countries. Moreover, by enhancing data streams the activities these associations are supporting are serving to furnish groups with data on issues, for example, maternal consideration, family planning and maternity care.
In ICT, “information” is focal that begins from gathering a beginning from information and moving towards learning. In spite of the fact that “information” gives no judgment or elucidation, it is vital crude material for the formation of information which is vital for compelling information administration in any electronic improvement activities especially in the health sector (Nemeth, Wears, Patel, Rosen & Cook, 2011).
In developing countries, a high toll rate is still incurred apart from preventable infections and unexpected losses. Disparity of access to fundamental healthcare influences distinct locales, groups, and social gatherings. Under-financing of the health division in many nations has prompted quantitative and subjective insufficiencies in service and to the increasing gaps in equipment and facility upkeep. Wasteful portion of rare assets and absence of coordination among key partners have endeavoured duplication of endeavours, covering obligations, and asset wastage regular and troublesome issues. Most nations are at some phase of health segment change, attempting to give extended and even-handed access to quality administrations while lessening or possibly controlling the increasing expense of human services. Health change procedures have numerous aspects and there is no single model being received by all nations (Courtney, Shabestari & Kuo, 2013).
ICTs can possibly make a noteworthy commitment to enhancing access and nature of services while containing expenses. Enhancing health includes enhancing general health and medicinal projects intended to give elective, crisis, and long haul clinical consideration; instructing individuals; enhancing nourishment and cleanliness; and giving more sterile living conditions. These thusly at last include gigantic social and monetary changes, the same number of health difficulties go well past the health segment. The health part has constantly depended on innovations. As indicated by Berger & Adedeji (2013), they shape the foundation of the administrations to avert, analyse, and treat sickness and ailment. ICTs are stand out classification of the immeasurable cluster of innovations that may be useful. Given the right strategies, association, assets, and organisations, ICTs can be effective apparatuses in the hands of those attempting to enhance health (Belkin, Corbitt & Wickramasinghe, 2013).
The routines individuals’ utilisation to speak with one another has additionally changed altogether. Portable telephony, electronic mail and videoconferencing offer new choices for sharing points of view. Computerised innovations are making visual pictures and the voices of individuals more available through radio, TV, feature, convenient plate players and the Internet, which change the open doors for individuals to impart insights, experien bankrupted groups to get to benefits and draw in with and request a health division that reacts to their needs and needs is impacted by more extensive information and correspondence procedures introduced by ICTs.
Role of ICTs in Developing Countries
Health is the core component of human beings and all the human beings have their civil rights on maintain their health in order to acquire a normal and healthy life. Health is fundamental to the worldwide plan of lessening destitution and in addition an essential measure of human improvement (Kabene, 2010). The main roles served by the ICT which are specifically health related are as follows:
- Reduce infant mortality
- Improve maternal health
- Combat HIV and AIDS, jungle fever, and different infections
Alternate ICTs incorporate health related targets and reflect a large number of the social, monetary, natural, and sexual orientation related determinants that have an effect on individuals’ health. Accomplishing them will likewise add to upgrades in the health status of a great many individuals around the globe. These objectives include:
- Abolishing hunger and poverty on extreme
- Enhancing knowledge and education;
- Authorising and appraise learning skills in women
- Developing water and sanitation frameworks;
- Developing universal organisations (in addition to other things to enhance access to reasonable, key medications on a manageable premise).
The ICTs does not work in separation and thusly they cannot be dealt with in disconnection. The policy efforts and exchanges need to consider the more extensive health determinants that influence individuals’ lives (Nomoto, Utsumi, Sasayama & Dekigai, 2014). Saranummi (2005), for instance, has built up an applied model for children diseases and mortality that considers the political, financial, and social frameworks that decide how assets are utilised and controlled. This serves to recognise the number and conveyance of youngsters who does not have adequate access to nourishment, child consideration, clean water, sanitation, and healthcare. This kind of examination is appropriate to other general health issues, for example, AIDS, or women’ health (Courtney, Shabestari & Kuo, 2013). Unless assets are additionally dedicated to handling the more extensive determinants of health, more health spending improves health (Issel, 2010).
ICTs need to work in collaboration with whatever other arrangement activities or methods, for example, national destitution reduction ystems (Finnegan & Currie, 2008) or as a major aspect of national health strategies. Numerous improvement establishments have investigated the association in the middle of ICTs and efforts to lessen destitution and accomplish alternate MDGs, including the Organisation for Economic Cooperation and Development (Kabene, 2010), the U.K. Office for International Development (Nomoto, Utsumi, Sasayama & Dekigai, 2014), and the Swedish International Development Cooperation Agency (Tamburis, 2006). The fundamental finish of these and different studies is that ICTs, when consolidated adequately into advancement projects can be helpful apparatuses in endeavours to achieve the MDGs.
Saranummi (2005) contends that there is developing proof of the capacity of ICTs to:
- Give new and more effective strategies for generation;
- Bring already unattainable markets inside of the span of poor people;
- Enhance the conveyance of taxpayer driven organisations;
- Encourage administration and exchange of information.
SIDA includes that, undeniably, samples can be discovered “where the utilisation of ICTs has notably tended to different parts of neediness. In spite of the different pitfalls connected with sending ICT ventures, developing proof the utilisation of ICTs can be a discriminating and obliged segment of tending to a few features of destitution. It is clear that ICTs themselves won’t kill poverty, however it is just as clear that numerous parts of destitution won’t be annihilated without the well-thoroughly considered out utilisation of ICTs.” (Nomoto, Utsumi, Sasayama & Dekigai, 2014) in the meantime, it is troublesome, if not outlandish, to build up ‘”demonstrated experimental connections” between the utilisation of ICTs and the accomplishment of the MDGs. As the Nemeth et. al (2011) focuses out: ‘Measuring the effect of ICT on health by and large is by all accounts genuinely troublesome in light of the fact that there are clearly numerous different components that effect health’.
Role of ICTs in Developed Countries
As indicated by WHO, the utilisation of ICTs in health is not simply about innovation (Berger & Adedeji, 2013), but rather an intends to achieve a progression of sought results, for example,
- Health specialists settling on better treatment choices;
- Hospitals giving higher quality and more secure consideration;
- People settling on educated decisions about their own particular health;
- Governments turning out to be more receptive to health needs;
- National and nearby information frameworks supporting the improvement of powerful, proficient, and fair health frameworks;
- Policymakers and the general population turning out to be more mindful of health dangers;
- People having better access to the information and information they requirement for better health.
Plainly each of these columns can profit by the utilisation of ICTs. By and by, the utilisation of ICTs in the health division has had a tendency to concentrate on three general classifications that fuse these columns:
1. Enhancing the working of health care systems
By enhancing the administration of information and access to that information, including:
- Management of logistics of patient consideration,
- Administrative frameworks;
- Patient records;
- Ordering and charging frameworks
2. Improving the health care service
By better finding, better mapping of general health risks, better preparing and sharing of information among health specialists, and supporting these health workers in essential human services, especially rural health care, including:
- Biomedical writing inquiry and recovery;
- Telemedicine and remote analytic support;
- Continuing proficient advancement of health specialists;
- Diagnostics
- Critical support systems for decision;
- QA (Quality Assurance) systems;
- Disease observation and the study of disease transmission
3. Enhancing correspondence on health-care.
This incorporates enhanced information streams among health specialists and the overall population, better opportunities for health advancement and health correspondence; and enhanced criticism on the effect of healthcare and mediations, including:
- Patient information,
- Interactive correspondence,
- Media approaches,
- Health research
- Advocacy to enhance administrations.
Case of Evidence
The design-reality gap framework helps in measuring any distinctions that exist between the venture’s introductory configuration designs and current reality. The following diagram is a depiction of design-reality gap:
A design-reality gap analysis is useful in providing a commitment in re-designing the process which was practiced prior to the initial stage. The gaps highlight the key and specific problem areas which differ from the original design in reality. Therefore, it is used to inquire the lacking areas. It helps to better analyse the system and implement the newly made changes accordingly.
– Design
– Reality
– Gap
– Reality
This structure paper draws on learning to create direction and to recognise gaps. As indicated by Courtney, Shabestari & Kuo (2013), “health technologies are usually evidence ased when they meet all around characterised details and have been approved through
controlled clinical studies or lay on a broadly acknowledged accord by specialists.”
In Bangladesh, a task with an alternate scale was created to enrol, calendar, and track vaccination of youngsters. Situated in the city of Rajashahi, an electronic framework was acquainted with supplant a manual record-keeping framework (Garets & Horowitz, 2008).
More than a time of three years, the new framework had the capacity expand inoculation rates from around 40.43 % to more than 80.35 % (Finnegan & Currie, 2008). A discriminating purpose behind the venture’s prosperity was that it was intended to meet the intrigues and
needs of different partners, and to furnish them with substantial advantages. The undertaking decreased the time health specialists spent seeking records; made it less demanding for administrative staff to oversee the inoculation framework and screen execution; and enhanced
vaccination assurance for youngsters and eventually their health, profiting every one of the families came to by the framework.
The design-reality gap analysis in the case of evidence is shown below:
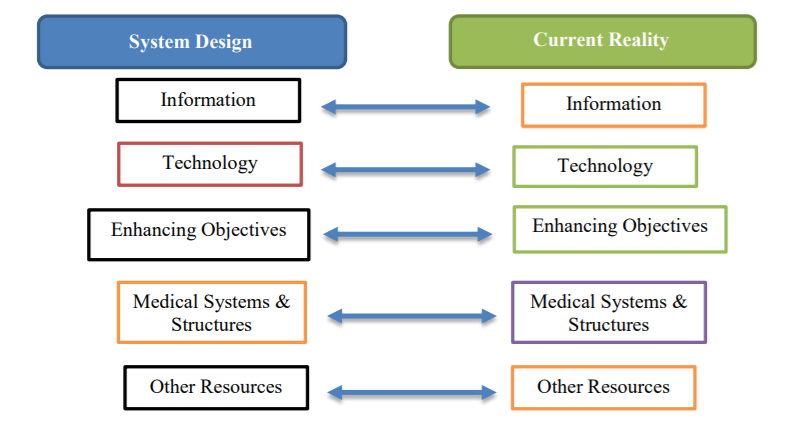
In this particular ICT initiative, significant design-reality gaps were identified in relation to:
- In the above design-reality gap analysis, it can be analysed that the flow of information has gaps within the country. This is due to the external factors which act as barriers and restrict ICT to serve better and thus leave a gap.
- The developing countries have technological gaps as ICT being practiced in developed countries follow advanced technological systems as compared to the developing countries where technologies come late and create communication gap.
- The objectives being set by the ICT shall be revised and enhanced on a timely manner which still leaves a gap from the prescribed design.
- The medical systems and the infrastructure have a lot ground of improvement in the developing countries and yet leave a challenge for ICT to implement further improved system within the country.
- Other resources are additional resources which definitely have a need yet they are not available or scarce within the region yet leaving a gap from the original design in reality.
The gaps explained above demonstrates that the ICT system is effective yet they need improvement in order to fill those gaps within the country where the systems are being utilised and followed. It can also be said that ICT systems are not institutionalised properly
within the government.
The analysis helped in determining two key areas which includes the explanation of the presence of minor gaps that were queued behind the limited success of the system and it explained to look into the experiences and policies needed to run ICT system. This may consist of introducing new technologies, new structure or enhancing the flow of information in order to ensure stability within the system (Berger & Adedeji, 2013).
Crucial to the viable utilisation of ICTs is the idea of included worth – all members must escape from an information framework in any event as much as they put in. The framework must create advantages more noteworthy than its cost; else it turns into a weight. Information frameworks are absolutely indigent upon the staff that give and record the information, yet the staff is typically the most reduced esteemed and minimum included. On the off chance that the advantages of their commitment are not clear to the staff, there is a high likelihood of building mistake, unsteadiness, and future failure (Garets & Horowitz, 2008).
It is imperative to recall that the setting in which ICTs in health care frameworks work, the clinical examples they bolster, and the approach environment will all change continually, and the information frameworks must react to these progressions. New opportunities will emerge, which ought to be misused when money saving advantage examination demonstrates this to be legitimised. Checking and assessment of information frameworks and other ICT intercessions empowers acclimations to be rolled out as per how the improvements are seen, and how they change practices.
Health specialists included in essential human services in developing countries are regularly segregated. They work in remote settings, frequently alone, and have almost no mode of accessing information and chances to trade encounters with partners. This circumstance is starting to enhance as health workers improve utilisation of existing innovations and figure out how to utilise new advances. In Ghana, Kenya, and Uganda, Satellife has been building background around the utilisation of PDAs (little handheld gadgets) that empower health workers in remote settings to obtain entrance to information; catch, store and offer critical health information; and connection to the encounters of different partners to enhance their practices and the results for their patients (Kabene, 2010).
There are two strong messages which can be incurred by the experience highlighted in this area. There is a need to guarantee that ICT use in the health division contacts the poorest populaces and there is an in number concentrate on connecting country, remote, troublesome situations that are underserved with the assets that are situated in the focal healthcare. Issel (2010) contend that guaranteeing that individuals living in country ranges are the real recipients in ICT activities will help meet the MDGs including those identified with health. Nonetheless, a late Food and Agricultural Organisation (FAO-2003) report brings up that “there has been for all intents and purposes no advancement in making the Internet accessible at all created nations, particularly in the provincial regions.” More MDGs can be tended to by incorporating rustic populaces in the gathering of recipients of ICT activities in the health sector, as the country poor constitute the most powerless populace bunch. Around 75 %of the world poorest live in country zones. Health conditions in provincial regions are by and large poorer, and access to information, administrations and supplies is generally constrained (Belkin, Corbitt & Wickramasinghe, 2013). Actualising ICT initiatives most likely means empowering go-betweens, for example, NGOs, health teachers, scholarly organisations, or nearby business visionaries, to go about as conductors for information accessible by means of innovations, for example, the Internet, and poor people, through interpretation, adjustment and utilisation of more conventional method for correspondence (Saranummi, 2005).
A portion of key lessons in this brief survey of the writing and investigation about the role and capability of ICTs it serves in health care frameworks is as follows:
- A successful way to deal with setting up information frameworks is to expressly recognise
- the destinations of the framework and focus the normal results.
- For most extreme potential achievement, an ICT task obliges all members (from the
- designers of the framework to the clients and recipients) to see the development as increasing
- the value of existing frameworks. In the event that the individuals utilising the framework
- don’t care for, need, or bolster it, it will probably come up short.
- Information frameworks ought to never get to be static or they will lose their worth.
References
Belkin, M., Corbitt, B., & Wickramasinghe, N. (2013). Strategic ICT planning in pathology. New York, NY: Springer.
Berger, H., & Adedeji, N. (2013). Challenges of adopting ICT solutions in a Nigerian healthcare SME. IJMP, 6(1), 77. doi:10.1504/ijmp.2013.052318
Courtney, K., Shabestari, O., & Kuo, A. (2013). Enabling health and healthcare through CT.
Finnegan, D., & Currie, W. (2008). A Centrist Approach to Introducing ICT in Healthcare. Journal of Cases on Information Technology, 10(4), 1-16. doi:10.4018/jcit.2008100101
Garets, D., & Horowitz, J. (2008). Healthcare ICT in Europe: Understanding trends in adoption and governance. Journal of Management & Marketing in Healthcare, 1(3), 286-296. doi:10.1179/mmh.2008.1.3.286
Issel, L. (2010). Health Care Reform Implications for Health Care Administration Science and Practice. Health Care Management Review, 35(2), 103-104. doi:10.1097/hmr.0b013e3181d3c21c
Kabene, S. (2010). Healthcare and the effect of technology. Hershey, PA: Medical Information Science Reference.
Nemeth, C., Wears, R., Patel, S., Rosen, G., & Cook, R. (2011). Resilience is not control: healthcare, crisis management, and ICT. Cognition, Technology & Work, 13(3), 189-202. Doi: 10.1007/s10111-011-0174-7
Nomoto, S., Utsumi, M., Sasayama, S., & Dekigai, H. (2014). P308: The effectiveness of ICT tools for sharing home healthcare information: Which patients and healthcare professionals would benefit most? European Geriatric Medicine, 5, S178. Doi: 10.1016/s1878-7649(14)70472-3
Saranummi, N. (2005). Regional health economies and ICT services. Amsterdam: IOS.